



Difference Between Asthma and COPD: Key Differences You Should Know


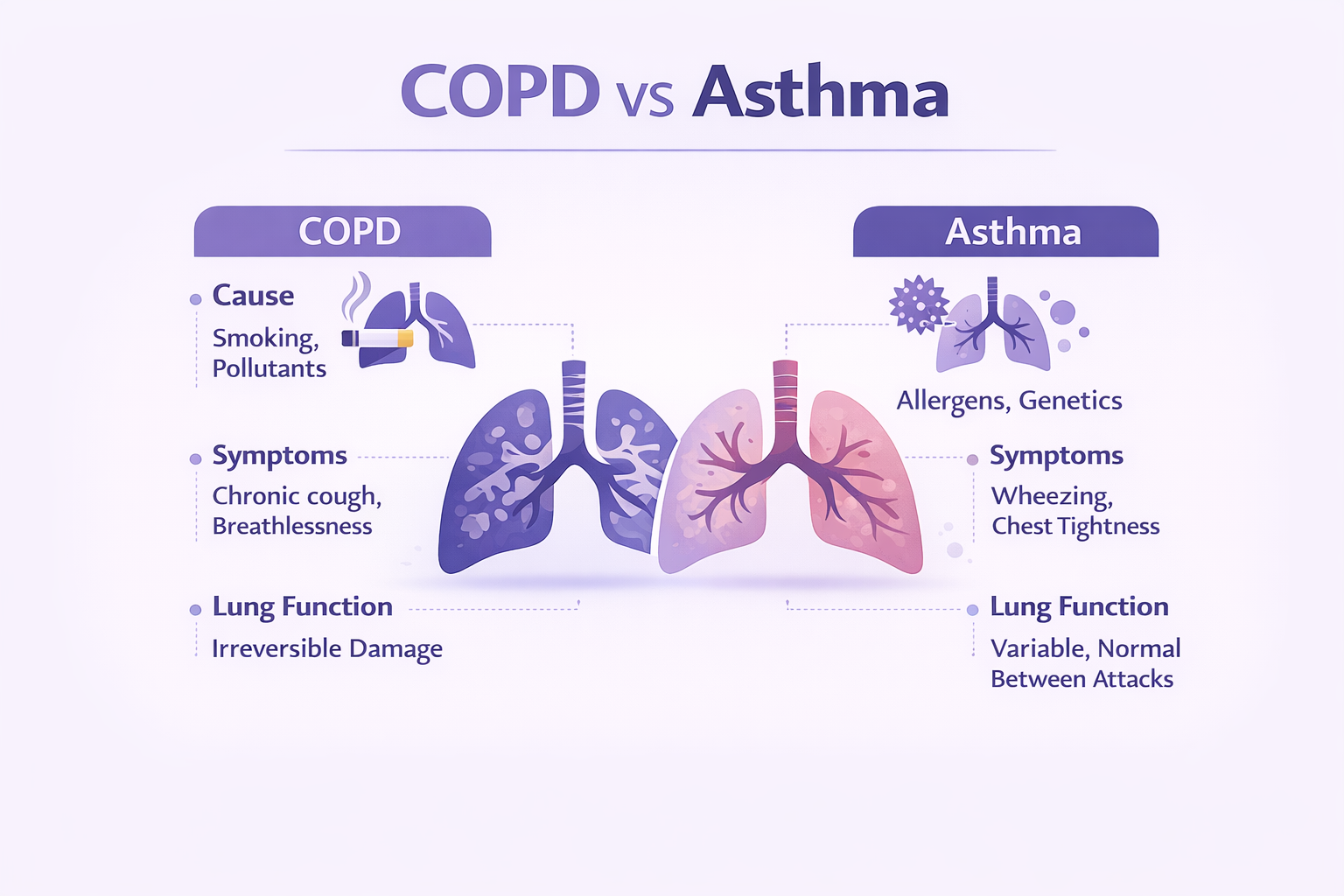
Table of Contents
Introduction: Understanding Two Common Lung Conditions
Many times, breathlessness, wheezing, or persistent cough sends people down an online rabbit hole of "asthma vs COPD” searches. While both diseases restrict your airways, their causes are poles apart. Asthma is not restricted to any age; it affects people of all ages, including children. It is usually an allergic disease that results in reversible spasms of the respiratory tract. On the other hand, chronic obstructive pulmonary disease is a progressive disease that can be caused by chronic smoking or inhalation of biomass smoke or chullah smoke. This post provides the difference between asthma and COPD, covering their symptoms, causes, and everyday management techniques.
Around 250 million individuals worldwide are affected by asthma., wWhereas COPD is the fourth most common cause of death worldwide. Together, asthma and COPD result in nearly 4 million deaths annually. 90% of these deaths are avoidable and happen in low- and middle-income nations.
Asthma vs COPD: Key Differences
While both asthma and COPD are chronic inflammatory lung diseases, they are completely different disorders. A hyper-responsive immune system drives asthma; consider airways that overreact to innocuous triggers including pollen, pet danger, dust, or a vigorous run. Usually beginning in childhood and leaving long symptom-free intervals between flare-ups, the outcome is temporary, reversible narrowing.
Chronic obstructive pulmonary disease, or COPD, presents quite a different picture. Years of toxic exposure—mostly coal, wood-fire "chulha," smoke and industrial dust—slowly scar and destroy the air sacs here, most usually from cigarettes. Usually starting after age 40, symptoms include thick phlegm, a daily "smoker's cough," and breathlessness from walking across the room to stair climbing.
| Feature | Asthma | COPD |
|---|---|---|
| Typical age at start | Childhood or teens (can start at any age) | > 40 years, after long-term exposure of causative agents |
| Main driver | Allergic or irritant triggers set off aggressive immune reaction. | Damage from tobacco, biomass smoke, industrial pollutants. |
| Airway narrowing | Reversible with reliever inhaler or steroids | Partly irreversible—structural lung damage limits full recovery |
| Symptom pattern | Episodic coughing (at night or with exercise), wheezing, and chest tightness, often triggered by allergens or physical activity. | Daily breathing difficulty and morning coughing with phlegm |
| Flare triggers | Pollen, pets, viral colds, cold air, exercise | Chest infections, continued smoking, winter smog |
| Long-term outlook | Usually stable if triggers avoided and inhalers used correctly | Gradual decline; can be slowed but not reversed |
| Classic preventive step | Allergen avoidance + inhaled corticosteroid | Quit smoking + pulmonary rehab |
| Overlap possibility | Asthma–COPD overlap seen in older smokers with childhood asthma history |
It is important to differentiate between asthma and COPD for appropriate treatment. Understanding the differences between asthma and COPD might help you discuss your symptoms better with your healthcare provider. In turn, accurate diagnostic tests are chosen by the treating doctor, and appropriate medicines are prescribed to manage your condition.
Symptoms: Overlapping Yet Distinct
| Symptom | Asthma | COPD |
|---|---|---|
| Wheezing | Often at night, early morning, or following a sprint, loud, musical wheeze that originates in sudden bursts | Possibly present, but less whistly; many COPD sufferers claim more "chest crack-les" than actual wheezing. |
| Breathlessness | Usually brought on by allergies, cold air, exercise, or stress, shows in brief, dramatic episodes often quickly corrected with a reliev | Climbing stairs or shopping the market could feel like a marathon; gradually, daily shortness of breath gets worse over years. |
| Cough | Usually dry and irritable; flares at night or following dust or pollen exposure. | Constant "smoker's cough" in the morning especially that brings up sticky mucus. |
| Variation in symptoms | High variability: many days free of symptoms between asthma bouts | Low variability: symptoms show consistent decline instead of sudden changes |
| Common triggers | Typical causes are pollen, pet fur, viral colds, high trigger sensitivity exercise | Cigarette smoke, biomass fumes, winter smog, chest infections (damage already present) |
Diagnostic Approach: How Tests Help Tell Them Apart
Telling asthma from COPD starts with good detective work—a chat about your symptoms and exposures—then moves to objective lung tests that show exactly how and why your airways are struggling.
| Diagnostic Tool | What It Checks | Typical Asthma Finding | Typical COPD Finding | Why It Matters |
|---|---|---|---|---|
| Spirometry | Your FEV?, FVC, how quickly and how much air your blow out | Big jump (? 12 % & 200 mL) in FEV? following a bronchodilator—proof of reversibility | Little or no change following a bronchodilator—airflow limitation is fixed | First-line test for asthma vs COPD diagnosis |
| Bronchial Provocation also known as Methacholine Challenge | “twitchiness” in aiways | Airways narrow at very low doses—high hyper-responsiveness | Usually either normal or only minor constriction | Applied when spirometry shows normal, but asthma still suspected |
| Full Pulmonary Function Test (PFT) | Lung volumes and gas transfer | Volumes usually normal between attacks; diffusion (DLCO) normal | Air trapping, high residual volume, low DLCO in advanced disease | Severity of disease and for long term care plan |
| X-ray / CT scan of chest | Structure of the lungs and diaphragm shape | Typically normal; occasionally, during a bad attach, possible transient hyperinflation during a bad attack | Hyper-inflated lungs, flat diaphragm | Helps in ruling out infection etiology, heart disease, and highlights COPD vs asthma pathology |
| Blood tests | Risk related to Inflammation or genetic | Elevated eosinophils or IgE point to an allergic pattern | Test for alpha-1 antitrypsin deficiency in younger COPD cases | Aids in customizing inhaler selection and spot rare causes |
| Symptom or Peak-Flow Diary | Day-to-day change in airflow | Big ups & downs (at least 20 %) indicates asthma | Numbers remain low and flat | Simple home tool to document asthma vs COPD airflow variation |
It is important for you to consult your doctor before taking any of these tests. They will prescribe the necessary tests for you and also explain any precautions to be taken or any medications to take/ stop before the tests.
How doctors put the puzzle together
- History first: childhood allergies or pet triggers raise asthma flags; decades of smoking steer toward COPD.
- Spirometry with reversibility is the cornerstone—one five-minute blow test can distinguish a flexible asthmatic airway from a stiff COPD airway.
- Provocation tests (methacholine) catch “hidden” asthma when baseline results look normal.
- Imaging either helps in ruling out surprise culprits like heart failure or tuberculosis or confirms lung damage due to COPD.
- Targeted blood work fine-tuned treatment: high eosinophils signal steroid-responsive asthma; low alpha-1 antitrypsin betrays a rare genetic COPD.
Combining these hints will help your doctor to decide which inhaler and which strength of inhaler to use. Also, it helps them to decide whether medicines for allergies are needed.
Treatment Differences: Managing Asthma vs COPD
Since the problems in the lungs caused by asthma and COPD are different, they need separate management plans.
| Management Area | Asthma | COPD |
|---|---|---|
| Main Goal | Calm airway inflammation & stop sudden attacks | Slow lungs decline & ease everyday breathlessness |
| Core Medicines | Inhaled corticosteroid (ICS) daily; your doctor might add a Long-acting bronchodilator (LABA) if symptoms persist | Long-acting bronchodilator (LAMA or LABA) is first-line; add ICS only for frequent flare-ups or high eosinophils |
| Quick-Relief Inhaler | SABA (e.g., salbutamol) for immediate wheeze control | Short-acting anticholinergic or SABA for rescue, but effect is mild. |
| Rehabilitation | Usually not required if asthma is well-controlled | Pulmonary rehab—exercise training, breathing techniques, nutrition advice—improves stamina & quality of life |
| Lifestyle Focus | Avoid or reduce triggers: dust, pollen, pets, strong smells | Quit smoking, avoid exposure from biomass-fume, use masks during winter |
| Vaccinations | Annual flu and pneumococcal vaccines to reduce attack risk | Same vaccines; pertussis booster recommended in some guidelines |
Common must-dos: Stay physically active, eat a balanced and healthy diet as recommended by your doctor, and see your doctor if rescue inhalers are needed more than twice a week.
Conclusion
Asthma and COPD are both diseases of the lungs; however, both are different. They have different causative factors, symptoms, and management strategies. COPD is a long-term long damage to the lungs whereas asthma is often reversible, driven by triggers. Spirometry, noting symptoms, and the appropriate scans can help in identifying the condition that you might have. This helps doctors to prescribe appropriate inhalers and suggest lifestyle changes. Know the difference, work with your doctor, and you’ll breathe easier, dodge flare-ups, and protect your lungs for the long haul.
References
Asthma and Chronic Obstructive Pulmonary Disease (COPD) - Medical Archives (PMC3633485)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3633485/
Global Initiative for Asthma (GINA)
https://ginasthma.org/
Global Initiative for Chronic Obstructive Lung Disease (GOLD)
https://goldcopd.org/
Comparison of clinical features and management of asthma and COPD - European Review for Medical and Pharmacological Sciences
https://www.europeanreview.org/wp/wp-content/uploads/1495-1510.pdf
Disclaimer
This content is intended for general educational and informational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment.
Rate the article

Comments